



Mental health as a risk factor for ESL: diagnostics, prevention, intervention
Thursday 23 July 2015, by
Mental health problems (e.g. anxiety, depression) are some of the risk factors for ESL and, by focusing on mental health prevention and intervention programmes in the school environment, we can reduce the many negative consequences poor mental health has on both the individual and community levels.
ESL is a complex long-term process involving multiple environmental, psychological and academic factors. There is increasing recognition of the need to recognise the role of mental health in educational processes (including in ESL). Studies investigating whether common mental disorders indeed constitute relevant risk factors for early school leavers have provided little consistent evidence. In the paper, we focus on internalisation problems (e.g. anxiety and depression) and externalisation problems (e.g. aggression) as well as the mechanisms linking them to lower academic achievement and ESL. The underlying mechanisms of mental health problems associated with low achievement are related to lower connectedness to school, negative attitudes to school, and peer rejection (in case of aggression and disruptive behaviour disorders), lower engagement through impaired mastery beliefs and negative emotionality (as in the case of depression) and difficulties with cognitive functioning through reduced memory functions and the impact of worries on the cognitive system (as in the case of anxiety). The relationship between mental health problems and school performance is two-directional. Mental health problems can precede problems related to school performance and, on the other hand, difficulties in school can result in various problems with mental health. In the paper, the importance of early recognition, assessment and later on prevention and intervention (on universal, selective and individual levels) is stressed. The findings are based on a review of the relevant literature. The need to clearly establish a relationship between anxiety and ESL is especially relevant since the research shows that anxiety levels are on the increase in school-aged populations (Kozina, 2014; Twenge, 2000). The studies in the EU (Angermeyer et al., 2004) which reveal that a high proportion (13.6%) of 18-year-olds have anxiety disorders make the topic even more pertinent.
Mental health and school functioning (their role in ESL)
A diagnosis of psychopathology in adolescence is frequently preceded by difficulties in academic and social functioning (Boyce, Essex, Woodward, Measelle, Ablow, & Kupfer, 2002). Roderick and colleagues (Roderick, Eggert, Thomson, Randell, & Pike, 2002) studied truancy and identified mental health problems as factors contributing to poor school attendance. Similarly, Eggert and colleagues (2002) identified an increased risk of depression among disengaged students prone to ESL. The relationship between mental health problems and school performance is two-directional. Mental health problems can precede problems related to school performance. This is usually related to physiological and cognitive changes due to mental health issues that interfere with the learning process (for instance, insomnia in depression, cognitive preoccupation with worries in anxiety) (Hishinuma et al., 2012). This means that a mental disorder can in itself significantly interfere with cognitive functioning and also be related to learning difficulties and ESL. On the other hand, difficulties in school can result in various problems with mental health. School is an important domain in which children achieve developmental milestones (DiSocio & Hootmen, 2004) and therefore a lack of success in this domain can lead to different mental health issues especially for students who attribute great significance to their academic achievement (Hishinuma et al., 2012). For instance, ESL students are more prone to different mental health problems (DiSocio & Hootmen, 2004) even when controlling for their mental health status prior to ESL (Kaplan, Damphouse, & Kaplan, 1994). Either way, the persistence of poor school functioning combined with a mental health problem can lead to school disengagement and ESL.
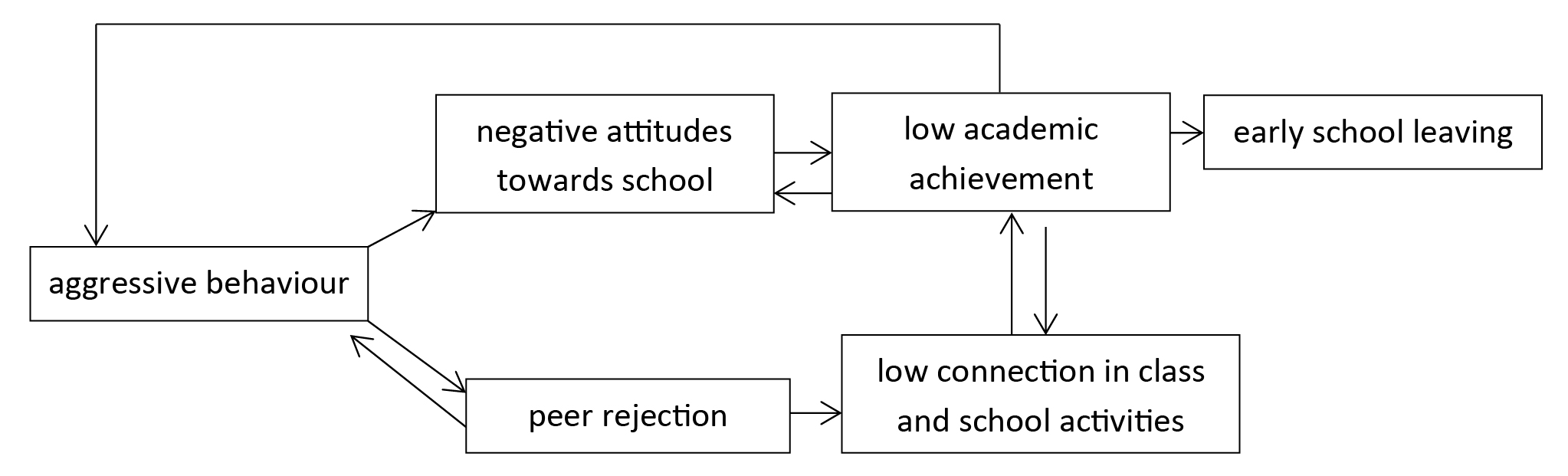
The most commonly mentioned mental health problems associated with school difficulties (and school failure) are externalisation disorders (disruptive behaviour disorders: attention deficit disorders, oppositional deviant disorder and conduct disorder) and internalisation disorders (anxiety and depression). As mentioned, we will focus more on depression and anxiety, but first we should point out that disruptive behaviour disorders (with aggression in their core) are related to problems in school functioning. Children with this type of disorders usually have difficulties with transitions, fitting into peer groups and forming friendships, which can lead them to associate more with deviant peer groups that are also prone to truancy and ESL (DiSocio & Hootmen, 2004; Battin-Pearson, Newcomb, Abbot, Hill, Catalano, & Hawkins, 2000). Research shows that aggressive behaviour in early childhood serves as a significant predictor of negative attitudes to school, which is also strongly related to lower academic achievement (Huesmann, 1994). Low academic achievement has consistently been one of the strongest predictors of dropping out of high school (Battin-Pearson et al., 2000). Further, the associations between aggression and the school climate (Flannery, Vazsonyi, & Waldman 2007) as well as between aggression and academic achievement (McEvoy & Welker 2000) are significant even when socio-economic status is controlled for. Indeed, these variables often reinforce each other. For instance, pupils who exhibit more aggression at an early age also develop a negative attitude to school, resulting in lower achievement (Zhou, Main, & Wang 2010), and are more commonly rejected by their peers (Flannery et al., 2007; Huesmann, 1994). Rejection by one’s peers is significantly and consistently associated with lower connectedness to the class, which is followed by low involvement in class and school activities (Buhs, Ladd, & Herald 2006; Ladd, Kochenderfer, & Coleman 1997; Wentzel & Asher 1995), which ultimately significantly predicts low academic achievement (Buhs et al., 2006; Ladd et al., 1997; Vandell & Hembree 1994) as seen in the diagram below.
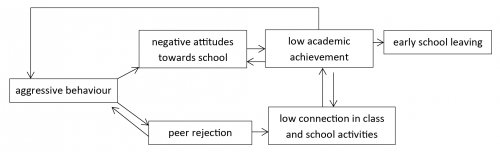
- Figure 1. Summary of the research findings – externalisation difficulties and ESL
Even though the depressive symptoms are not as noticeable as disruptive behaviour, they have a strong impact on one’s cognitive functioning and academic achievement. The school performance of depressed students is largely affected by poor concentration, distractibility, insomnia and day-time sleepiness, irritability and low self-esteem (DiSocio & Hootmen, 2004; Hishinuma et al., 2012). Studies have shown that self-reported depressive symptoms are negatively associated with self-reported academic competence and achievement and that these factors can undermine school performance (Quiroga et al., 2013). The relationship is mediated by students’ self-perception of academic competence. Even though ESL is a complex long-term process in which psychological factors (and mental health) play an important role, the mechanisms that link depression with ESL remain to be elucidated in research (Quiroga et al., 2013). Quiroga and colleagues (Quiroga et al., 2013), for instance, established that self-reported depression symptoms in Grade 7 increased the risk of ESL in later adolescence. Depressive individuals are prone to pessimistic ways of thinking with impaired mastery beliefs, leading them to believe they will not cope with school (Quiroga et al., 2013). Cross-sectional studies (Assarnow et al., 2005; Reinherz, Frost, & Pakiz, 1991) have shown that depressed youth are more likely to interrupt schooling. Longitudinal research shows some contradicting findings, namely, that depressive youth are more likely to leave school early but, when controlled for other ESL risk factors such as low academic achievement and family background, the path was no longer significant. It is therefore not yet clear whether depression has an effect on its own or depression is simply a result of the accumulation of various other risk factors (Ferguson & Woodwarth, 2002). Regarding this issue, Hishinuma and colleagues (2012) conducted a longitudinal study and established that depressive symptoms undermine academic success and not the other way around, indicating that depression on its own plays a significant role in education underachievement (and potential ESL). Another explanation is a link between depression and the low engagement of students. The negative emotionality that is characteristic of depressive students also impact engagement, e.g. by lowering positive emotions towards school and thereby diminishing the emotional component of engagement (Wang & Peck, 2013). Hishinuma and colleagues (2012) pointed out that emphasis must be given to screening, identifying and treating depressive symptoms and disorders, not only to reduce the ill effects but also to avoid low academic achievement.
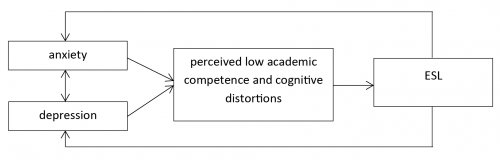
- Figure 2. Summary of findings – internalisation disorders and ESL
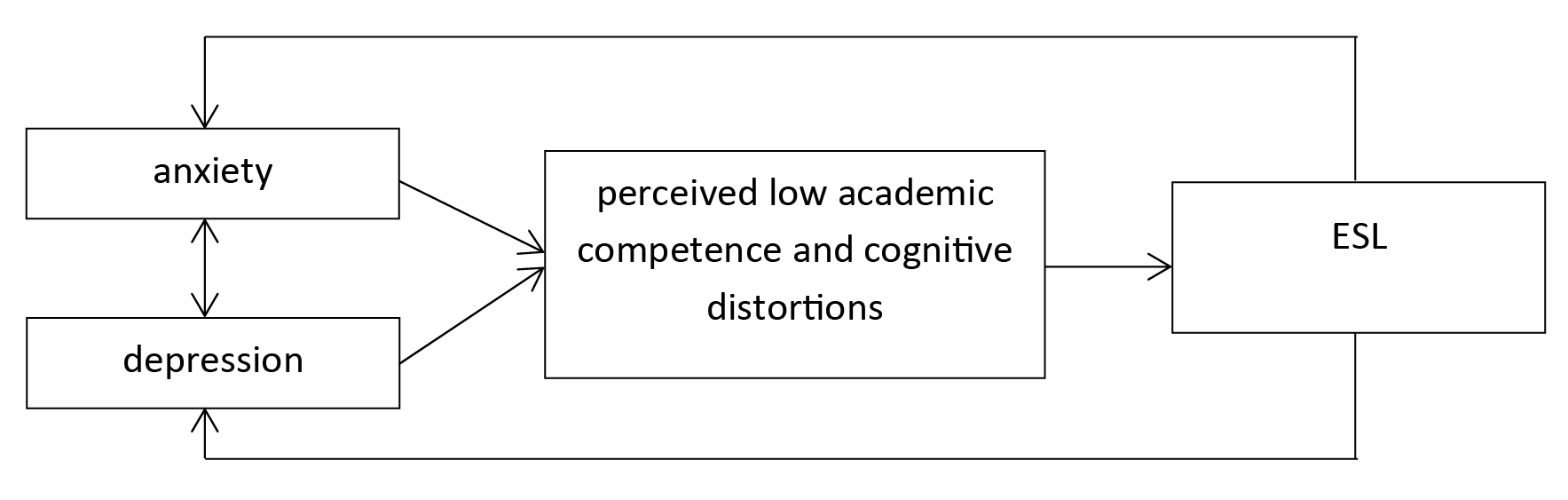
Depression and anxiety are frequently comorbid (sharing the common component of negative affect with increased activation in anxiety and decreased activation in depression (for details, see the Tripartite model of anxiety and depression, Chorpita, 2002)). Both anxiety disorders and depressive disorders contribute to school avoidance and academic underachievement (Woodworth & Fergusson, 2001). Anxiety is a cognitive, emotional, behavioural and physiological response of an individual experiencing a feeling of danger or threat, the cause of which they are not aware of (Fonseca & Perrin, 2001). High levels of anxiety, notably where clinical symptoms are expressed, interfere significantly with children’s adaptive functioning, social competence, peer relations and social adjustment (Last, Hansen, & Franco, 1997; Schwartz et al., 2006), and when present in childhood follow a chronic course, and continue into adulthood (Ialongo et al., 1996; Kim-Cohen et al., 2003; Woodworth & Fergusson, 2001). Anxiety is negatively correlated with educational achievement (Duchesne & Ratalle, 2010; Normandeau & Guay, 1998) in both clinical and non-clinical samples (Mazzone et al., 2007) and different age groups, i.e. at the primary and secondary levels of education (Mazzone et al., 2007). Students with higher levels of anxiety find it more difficult to learn new academic content (also related to learning difficulties), which may also be a result of reduced memory functions (caused by anxiety), making it difficult for them to complete cognitive tasks (Prevatt, Welles, Li, & Proctor, 2010). Cognitive theories highlight negative automatic thoughts (in the form of worries) that occur both during the learning process and the process of examination [1] as particularly disturbing (Anić, 2009). Studies have reported that 10% to 20% of underachieving students suffer from anxiety. Underachieving students are students who do not reach their potential in spite of adequate opportunities and abilities (they do not have learning difficulties). Studies have revealed that the influence can run in both directions. Reduced academic achievement leads to increased anxiety and, in turn, this increased anxiety results in reduced achievement because anxiety affects the processes of thinking and learning. Reduced academic achievement may lead to greater anxiety also due to the high expectations of parents. Parents’ expectations can occur in the form of negative thoughts (for instance, parental expectation in the form of the thought I have to get a good grade to get to a better school occupies the students while taking an exam) which occupy the working memory, thereby hindering the cognitive process (Hribar & Magajna, 2011). As mentioned, anxiety causes difficulties in learning even when learning deficits are not present. Thus, in cases where anxiety occurs among students with deficits in learning this poses an additional burden on cognitive processes, thereby further disrupting the acquisition of knowledge (Nelson & Harwood, 2011). Thus, high anxiety creates both short-term consequences (for instance, it interferes with the processes of reading and numeracy by burdening working memory) and long-term ones in the sense of poorer academic achievement and ESL (Hribar & Magajna, 2011).
The increase in anxiety holds significant implications for the mental and physical health of whole generations. It has been proven many times that high anxiety can, among others, cause intense psychosocial impairment (Silverman & Treffers, 2001) and lead to major depression, a wide variety of physical illnesses, impaired cognitive performance, marital problems and substance abuse (Twenge, 2000).
[1] As a result of cognitive impairment or a deficit in the field of learning some children develop a fear of examinations, which is associated with lower achievement.
Anić, N. (2009). Ocena študentov z učnimi težavami [Evaluation of students with learning difficulties]. In N. Anić (Ed.), Prispevki iz vedenjsko kognitivne terapije – zbornik 1 (257–266). Ljubljana: Društvo za vedenjsko in kognitivno terapijo Slovenije in Svetovalni center za otroke, mladostnike in starše.
Asarnow, J. R., Jaycox, L. H., Duan, N., LaBorde, A. P., Rea, M. M., Tang, L., … Wells, & K. B. (2005). Depression and role impairment among adolescents in primary care clinics. Journal of Adolescent Health, 37, 477–483.
Battin-Pearson, S., Newcomb, M. D., Abbot, R. D., Hill, K. G., Catalano, R. F., & Hawkins, J. D. (2000). Predictors of early high school drop-out: A test of five theories. Journal of Educational Psychology, 92, 568–582.
Boyce, W., Essex, M., Woodward, H. R., Measelle, J., Ablow, J., & Kupfer, D. (2002). The confluence of mental, physical, social, and academic difficulties in middle childhood. I: exploring the “headwaters” of early life morbidities. Journal of the American Academy of Child and Adolescent Psychiatry, 41(5), 580–587.
Boxer, P., Edwards-Leeper, L., Goldstein, S. E., Musher-Eizenman, D., & Dubow, E. F. (2003). Exposure to »low-level« aggression in school: Associations with aggressive behaviour, future expectations, and perceived safety. Violence and Victims, 18(6), 691–704.
Buhs, E. S., Ladd, G. W., & Herald, S. L. (2006). Peer exclusion and victimization: Processes that mediate the relation between peer group rejection and children’s classroom engagement and achievement? Journal of Educational Psychology, 98, 1–13.
Chorpita, B. F. (2002). The tripartite model and dimensions of anxiety and depression: An examination of structure in a large school sample. Journal of Abnormal Child Psychology, 30(2), 170–199.
DeSocio, J., & Hootman, J. (2004), Childrens mental health and school success. The Journal of School Nursing, 20(4), 189–196.
Downes, P. (2011). The neglected shadow: European perspectives on emotional supports for early school leaving prevention. The International Journal of Emotional Education, 3(2), 3–36.
Duchesne, S., & Ratelle, C. (2010). Parental behaviours and adolescents’ achievement goals at the beginning of middle school: Emotional problems and potential mediators. Journal of Educational Psychology, 120(2), 497–507.
Eggert, L. L., Thompson, E. A., Randell, B. P., & Pike, K. C. (2002). Preliminary effects of brief school-based prevention approaches for reducing youth suicide: Risk behaviors, depression, and drug involvement. Journal of Child and Adolescent Psychiatric Nursing, 15(2), 48–64.
Fergusson, D. M., & Woodworth, L. J. (2002). Mental health, educational and social role outcomes of adolescents with depression. Archives of General Psychiatry, 59, 225–231.
Flannery, D. J., Vazsonyi, A. T., & Waldman, I. D. (2007). The Cambridge handbook of violent behaviour and aggression. Cambridge: Cambridge University Press.
Fonseca, A. C. & Perrin, A. (2001). Clinical phenomenology, classification and assessment of anxiety disorders in children and adolescents. In W. K. Silverman & P. D. A. Treffers (Eds.), Anxiety disorders in children and adolescents (126–159). Cambridge: Cambridge University Press.
Fox, J. K., Herzig-Anderson, K., Colognori, D., Stewart, C., & Masia Warner, C. (2013). School-based treatment of anxiety in children and adolescents: New developments in transportability and dissemination (355–369). In M. D. Weist, N. A. Lever, C. P. Bradshaw, & J. S. Owens (Eds.), Handbook of school mental health. New York: Springer.
Hishinuma, E. S., Chang, J. Y., McArdle, J. J., & Hamagami, F. (2012). Potential causal relationship between depressive symptoms and academic achievement in the Hawaiian high school health survey using contemporary longitudinal latent variable change models. Developmental Psychology, 48, 1327–1342.
Greenberg, M. T., Domitrovich, C. & Bumbarger, B. (2000). Preventing mental health disorders in school-age children. A review of the effectiveness of Prevention Programs. Rockville: Center for Mental Health Services (CMHS) Substance Abuse Mental Health Services Administration U.S. Department of Health and Human Services.
Hribar, N. & Magajna, L. (2011). Prepoznavanje in diagnostično ocenjevanje učencev z učnimi težavami zaradi anksioznosti [Screening and diagnostic evaluation of students with anxiety-based learning difficulties]. In L. Magajna & M. Velikonja (Eds.), Učenci z učnimi težavami – prepoznavanje in diagnostično ocenjevanje (1212–1230). Ljubljana: Pedagoška fakulteta Univerze v Ljubljani.
Huesmann, L. R. (1994). Aggressive behaviour – current perspectives. New York and London: Plenum Press.
Ialongo, N., Edelsohn, G., Werthamer-Larsson, L., Crockett, L., & Kellam, S. (1996). The course of aggression in first-grade children with and without co morbid anxious symptoms. Journal of Abnormal Child Psychology, 24, 445–456.
Kaplan, D. D., Damphousse, J. R., & Kaplan, H. B. (1994). Mental health implications of not graduating from high school. Journal of Experimental Education, 62, 105–123.
Kim-Cohen, J., Caspi, A., Moffit, T. E., Harrington, H., Milne, B. J., & Poulton, R. (2003). Prior juvenile diagnosis in adults with mental disorder: Developmental follow-back of a prospective–longitudinal cohort. Archives of General Psychiatry, 37, 709–717.
Kos, A. (1990). Strah v šoli, strah pred šolo [Fear in school, fear of school]. Ljubljana: Svetovalni center za otroke, mladostnike in starše.
Kozina, A. (2014). Developmental and time-related trends of anxiety from childhood to early adolescence: Two-wave cohort study. The European Journal of Developmental Psychology, 11, 546–559.
Ladd, G. W., Kochenderfer, B. J., & Coleman, C. C. (1997). Classroom peer acceptance, friendship, and victimization: Distinct relational systems that contribute uniquely to children’s school adjustment? Child Development, 68, 1181–1197.
Last, C.G., Hansen, C., & Franco, N. (1997). Anxious children in adulthood: A prospective study of adjustment. Journal of the American Academy of Child and Adolescent Psychiatry, 36, 645–652.
Masten, A. S., & Motti-Stefanidi, F. (2009). Understanding and promoting resilience in children: Promotive and protective processes in schools. In V T. B. Gutkin & C. R. Reynolds (Eds.), The handbook of school psychology. Hoboken: Wiley.
Mazzone, L., Ducci, F., Scoto, M. C., Passaniti, E., D’Arrigo, V. G., & Vitiello, B. (2007). The role of anxiety symptoms in school performance in a community sample of children and adolescents. Retrieved from: http://www.biomedcentral.com/1471-2458/7/347.
McEvoy, A., & Welker, R. (2000). Antisocial behaviour, academic failure, and school climate: A critical review. Journal of Emotional and Behavioral Disorders, 8, 130–140.
Mifsud, C., & Rapee, R. M. (2005). Early intervention for childhood anxiety in a school setting: Outcomes for an economically disadvantaged population. Journal of American Child and Adolescents Psychiatry, 11, 996–1004.
Nelson, J. M., & Harwood, H. (2011). Learning disabilities and anxiety: A meta-analysis. Journal of Learning Disabilities, 44, 3–17.
Normandeau, S., & Guay, F. (1998). Preschool behavior and first-grade school achievement: The meditational role of cognitive self-control. Journal of Educational Psychology, 90, 111–121.
Prevatt, F., Welles, T. L., Li, H., & Proctor, B. (2010). The contribution of memory and anxiety to the math performance of college students with learning disabilities. Learning Disabilities Research in Practice, 25, 39–47.
Rinherz, H. Z., Frost, A. K., & Pakiz, B. (1991). Changing faces: Correlates of depressive symptoms in late adolescence. Family and Community Health, 14, 52–63.
Roderick, M., Arney, M., Axelman, M., DaCosta, K., Steiger, C., Stone, S., Villarreal Sosa, L., & Waxman, E. (1997). Habits hard to break: A new look at truancy in Chicago’s public high schools. Research brief. Chicago, IL: University of Chicago School of Social Service Administration.
Schwartz, D. J., Hopmeyer Gorman, A., Nakamoto, J., & Mckay, T. (2006). Popularity, social acceptance, and aggression in adolescent peer groups: Links with academic performance and school attendance. Developmental Psychology, 42, 1116–1127.
Silvermann, W. K., & Treffers, P. D. A. (2001). Anxiety disorders in children and adolescents. Research, Assessment and Intervention. Cambridge, England: Cambridge University Press.
Vandell, D. L., & Hembree, S. E. (1994). Peer social status and friendship: Independent contributors to children’s social and academic adjustment. Merrill-Palmer Quarterly, 40(4), 461–477.
Wang, M., & Peck, S. C. (2013). Adolescent educational success and mental health vary across school engagement profiles. Developmental Psychology, 49, 1266–1276.
Wentzel, K. R., & Asher, S. R. (1995). The academic lives of neglected, rejected, popular, and controversial children. Child Development, 66, 754–763.
Woodworth, L. J. & Fergusson, D. M. (2001). Life course outcomes of young people with anxiety disorders in adolescence. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 1086–1093.
Widoe, R. K., Martins, R. K. & McNeil, D. W. (2006). Anxiety disorders in ethnic minorities. Encyclopaedia of multicultural psychology. Retrieved from: http://sage.reference.com/multiculturalpsychology/article_n24.html
Wienke-Totura, C. M., Mackinnon-Lewis, C., Gesten, E. L., Gadd, R., Divine, K. P., Dunham, S., & Kamboukos, D. (2009). Bullying and victimization among boys and girls in middle school – the influence of perceived family and school contexts. Journal of Early Adolescence, 29, 571–609.
Twenge, J. M. (2000). The age of anxiety? Birth cohort change in anxiety and neuroticism. Journal of Personality and Social Psychology, 79, 1007–1021.
Quiroga, C. V., Janosz, M., Bisset, S., & Morin, A. J. S. (2013). Early adolescent depression symptoms and school dropout: Mediating processes involving self-reported academic competence and achievement. Journal of Educational Psychology, 105, 552–560.
Zhou, Q., Main, A., & Wang, Y. (2010). The relations of temperamental effortful control and anger/frustration to Chinese children’s academic achievement and social adjustment: A longitudinal study. Journal of Educational Psychology, 120, 180–196.